UPDATE 13/2/16: NHS Employers has sent more specifics about the contract out rendering this post somewhat inaccurate. Will be adjusting it soon.
UPDATE 14/2/16: now adjusted to take into consideration the specific changes NHS Employers sent out on 13/2/16 to junior doctors.
A significant component of the current dispute between Health Secretary Jeremy Hunt and junior doctors is pay. It is not the whole dispute.
Part of the new proposals involve a hospital ‘guardian’. The ‘guardian’ would be responsible for ensuring doctors do not breach their hours. Where they do, guardians would enforce financial penalties. (It’s really hard to Google ‘guardian’ and ‘junior doctors’ strike’ without just getting articles from the Guardian.)
However, they would be employed by hospitals; the conflict of interest between an employee deciding whether to fine his or her employer is obvious. As yet, this issue has not been addressed by government. The practical effect on hours worked that having a guardian will have is unclear.
There are many other issues too. However, the question for this post is, what are the differences in pay going to be?
I’m going to use the last full-time rota I was on as an example. (NB: this is not the same rota for the whole country.)
I’m going to be using ‘old’ to represent the system at the moment and ‘new’ to represent to prospective system. Using the term ‘current’ could get a bit confusing.
If you can’t be bothered look at the maths, just go to the end. There’s a section called, The punchline, which summarises the key numbers.
The old system
This worked via something called ‘banding’. If you Google ‘NHS banding’ you get the bands for nursing and other healthcare professions.
The old banding system for doctors looked like this:
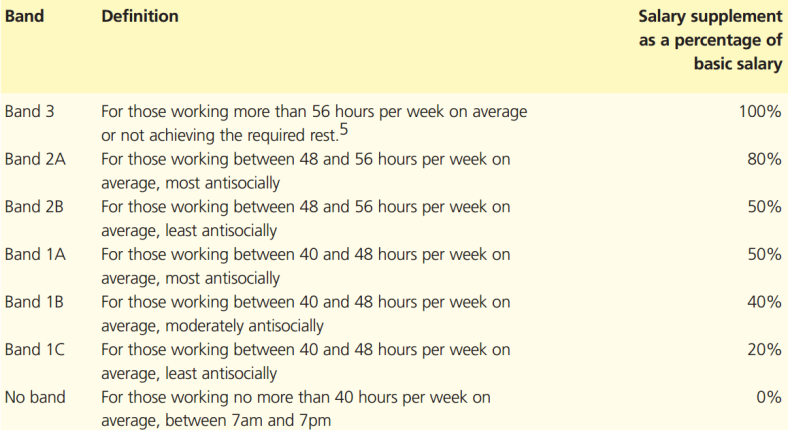
Are You Being Paid Correctly? p2 – The BMA
OH MY GOD WHAT EVEN IS THAT?
It looks complicated but the hospital tallies up the number of hours you’ve worked, the proportion that’s ‘antisocial’ and gives you a pay supplement based on that proportion.
Antisocial hours are considered the weekend and 1900-0700 during the week.
How do you figure out whether you’re moderately, most or least antisocial? You can use the following helpful chart:
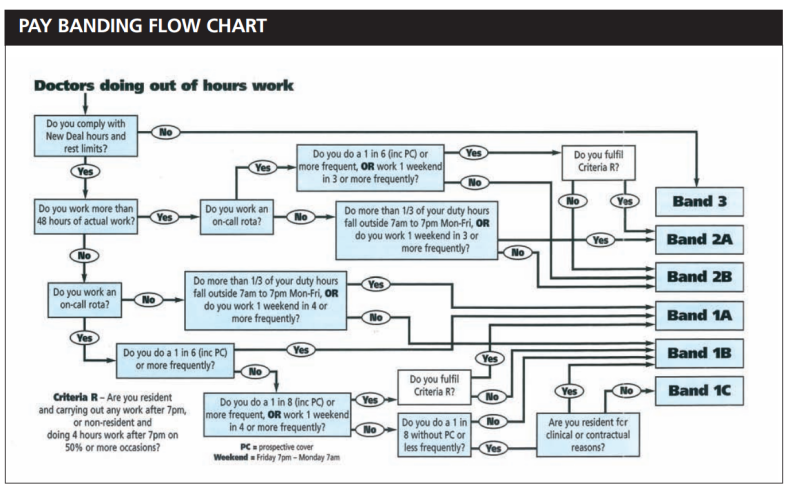
Are You Being Paid Correctly? p3 – The BMA
SERIOUSLY THEY ARE JUST TAKING THE MICHAEL NOW!
Suffice it to say, it’s fairly complicated. I say this with some trepidation but most first- and second-year doctors (F1 and F2 or Foundation Year 1 & 2) will be on 1A or 1B. I think.
This means, for the number of antisocial hours they work, they get a pay supplement of 40% of their basic salary.
The F1 year is usually split into 3 x 4-month placements. Assuming that all of these jobs have a fairly standard on-call rota for medicine or surgery, an F1 will receive a 40% supplement on the basic salary of £22,636
They’re paid 22636 x 1.4 = £31690 pa.
Placements vary. F1s often do jobs like medical microbiology or general practice which many only require social hours work – they do not receive a supplement for these jobs.
They may also work in emergency medicine (A&E) where they would receive an even bigger supplement but the shifts are largely antisocial.
The same applies to any hospital medic. They have a basic salary. The hospital calculates the proportion of antisocial hours; determines what band they’re in; and gives them the requisite pay supplement.
The key misunderstanding is that you get a percentage supplement on total hours under the old system, not just on the out-of-hours work as some of the press have suggested.
Now, I hope you enjoyed the arithmetic – there’s loads more to come.
The rise in basic pay
When I originally wrote this post, the government had been suggesting a 13.5% pay rise. Subsequently, NHS Employers have sent out this pay letter which has more specifics about the new pay scale. The old pay scale can be found here on the BMA website.
I’ve summarised them in this table:
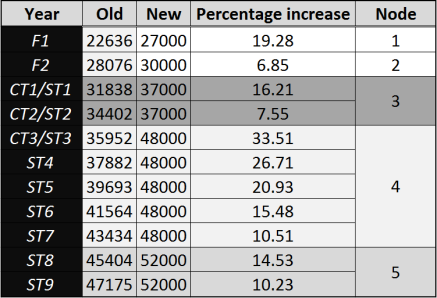
Pay and percentage increases relative to year
F1 and F2 refer to the first and second year of the foundation programme. If you look at the old pay scale, these consider pay for up to three years in each of these posts. These are relevant to part-time doctors which I’ve ignored, largely because it’s something I don’t have a lot of experience of.
CT/ST (core/specialty training) year refers to years in specialist training (surgery, internal medicine, pathology etc.). From the point of view of pay, the difference between core and specialty training posts is a technical one, not relevant here.
Otherwise, there are two changes. The first is simply there is an increase in basic salary across the board (though this doesn’t necessarily lead to a final salary increase).
Secondly, you’ll note the new ‘nodes’. Previously, there was a year -on-year increase in salary. Now doctors will have the same salary during certain blocks of training, particularly ST3-7.
Government argues that the responsibility of these doctors is the same regardless of grade. For anaesthetics and critical care, this is true when looking purely at on-call responsibility. However, it doesn’t consider the assessments and exams one has to pass to progress from year to year.
Most doctors require revalidation every 5 years. Junior doctors go through an equivalent process every year which is more onerous that revalidation.
How the new system’s supplements work
Oh, the fun I’ve had with this. My last job was as a CT2 anaesthetist. Looking at the table above, that means I would be paid 7.5% extra basic pay. I’ve also calculated my comparative pay as a CT1 anaesthetist which involves a 16.21% increase.
You can download the spreadsheet here but I’m going to use a couple of screenshots.
I’m not sure how well this will show up on whatever device you’re using. The top row is hours. 0700 means 0700-0800. I’ve put a ‘1’ for every hour I’ve worked and also to make the spreadsheet work.
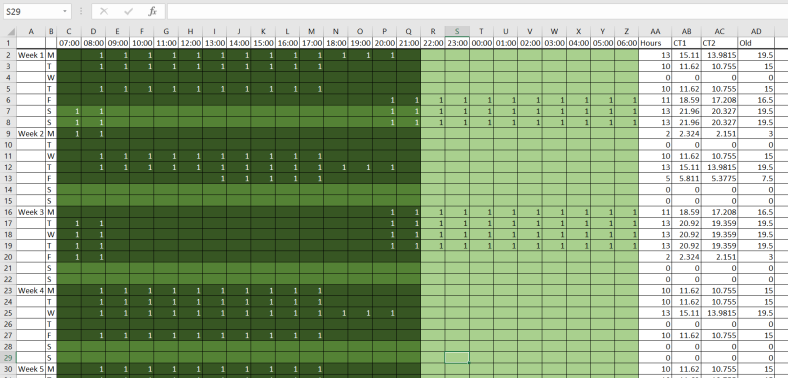
As a CT2, under the new contract:
- Basic hours, 0700-2100, Mon-Fri, +7.55% from the old system, dark green
- Saturday and Sunday, 0700-2100, +30% (on top of the 7.55%), middle green
- Antisocial hours, 2100-0700 Mon-Sun, +50% (on top of the 7.55%), light green (this says light green though you probably can’t see it)
(NB: if I were to work fewer the 1 in 4 Saturdays – I work 2 in 7 – I would get no supplement 0700-1700 on a Saturday which would further complicated payment. Also, it’s possible that because one of those shifts is day and one night, that they would be considered different shifts and I would not get a Saturday supplement. That would be pretty shifty.)
So you can see, the arithmetic gets a little complicated.
Broadly my job consists of three different types of shift:
- Normal day – 0800-1800
- Long day – 0800-2100
- Night – 2000-0900
There’s an hour overlap in the morning and evenings between the person coming and the person leaving. This is to facilitate handover. It doesn’t happen in every hospital but we got paid for it.
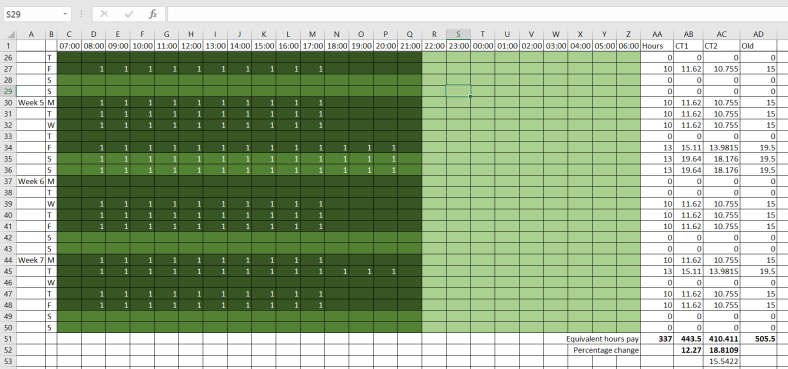
This is the bottom half of that spreadsheet. I was on a 1 in 7 rota. That means that there were 7 anaesthetists on the rota. Whilst I was on week 1, another was on week 2, another week 3 etc. This works out at 48.14 hours/week.
I should note, rota coordinators get a lot of stick in hospital but trying to design one of these things is hard. This one doesn’t show how, in order to be EWTD compliant (ie <48 hours/week), I have to get days off after weekend days and nights. Booking annual leave on top of that makes these things a nightmare.
In the ‘CT2’ column for Mon-Fri, I’ve used the following formula:
=1.0755*SUM(C2:P2)+1.5*1.0755*SUM(Q2:Z2)
That’s 1.0755 x the number of basic hours (to calculate the 7.55% pay rise) + 1.5 x 1.135 x the number of antisocial hours (to calculate the 7.55% pay rise and 50% antisocial hours supplement).
In the ‘CT2’ column for Saturday and Sunday I’ve used the following formula:
=1.3*1.0755*SUM(C7:P7)+1.5*1.0755*SUM(Q7:Z7)
That’s 1.3 x 1.0755 x the number of weekend day hours (to calculate the 30% supplement for weekend day hours and the 7.5% pay rise) + 1.5 x 1.0755 x the number of antisocial hours (to calculate the 50% antisocial hours supplement and 7.5% pay rise).
Phew!
In the bottom right, in box AA51, there is a number calculated from the formula
=SUM(AC2:AC50)
which is the sum of all the ‘CT2’ hours. I’ve done the same for CT1 except I’ve used the 1.1621 instead of 1.0755 (to indicate the 16.21% basic salary pay rise). This gives total equivalent hours of 443.51 and 410.411 respectively which I will explain shortly.
The old system – calculations
The ‘Old’column is a lot simpler because the supplement is added at the end. Every cell in the ‘Old’ column has the formula:
=1.5*SUM(C2:Z2)
which is 1.5 x the number hours worked that day (for the 50% banding supplement).
Then I’ve used:
=SUM(AD2:AD50)
to add up all the ‘old’ hours.
There is also an ‘hours’ column using:
=SUM(C2:Z2)
for each cell. This is simply to calculate the raw number of hours I worked without any supplementation. These are summed at the bottom of the column with:
=SUM(AA2:AA50)
How have I got more hours under the new system but I’m also working the same hours?
What I’ve calculated is my pay equivalent to basic hours under the old system. It is not the actual hours I worked but is way of comparing the different rates of pay.
The punchline
- I worked 337 hours in 7 weeks
- That’s 48.14 hours/week
- Under the old system, I was paid the equivalent of 505.5 old system basic hours with my 50% banding supplement
- Under the new system,
- At CT2 I was paid the equivalent of 410.411 old system basic hours with the plethora of supplement
- At CT1 I was paid the equivalent of 443.5 old system basic hours with the plethora of supplement
- That’s an 18% pay cut for CT2 and a 12.27% pay cut CT1
Now, you can’t just average the two pay cuts to get my total pay cut over two years. My pay was different for the two years under the old pay scale but hopefully this gives you an idea of the sort of cuts in pay we’re looking at.
There are caveats. There is a large variation between hospitals and an even bigger one between specialties. Surgeons’ rotas are different to anaesthetists’ rotas are different to medics’ rotas which are all different to the rota of a chemical pathologist.
Further, rotas will change. Given the new obligations, it is highly likely many hospitals will adjust their rotas meaning any sort of calculation based on new or old systems will be rendered irrelevant. That said, I doubt this particular anaesthetic rota will change very much. It already adheres to the new guidelines and it would be considerable hassle to change it.
This post isn’t making a judgement about whether it’s wrong. However, given the number of antisocial hours worked, I cannot fathom a situation where the acute specialties end up getting paid more unless the premiums are quite significant.
What I will say is I’m not sure how the new system is any simpler than the old system. Whatever. Maybe I’ll just go to Canada.
