Dominic Raab during his time at the Foreign Office.
Dominic Raab has resigned after Adam Tolley KC’s inquiry found that Raab’s behaviour whilst foreign secretary and justice secretary constituted bullying. Raab argued “that’s not bullying, and we can’t deliver for the British people if the bar is that low” in a BBC interview.
Is he right? Well…
No.
For a long time, there has been a perception that good leaders stand up at the front, assess the information, make a decision and their followers carry it out. If they make the correct decisions, they are good. If not, they are bad. It is a strongman approach to leadership.
This approach led to hundreds of people dying in plane accidents. Over half of fatal aviation accidents are due to human factors, the interaction between humans and complex systems. Aviation has for decades delivered human factors training to its staff.
Team members need to feel comfortable raising concerns and leaders need to listen to those concerns. When they do not, people die.
Compassion
Professor Michael West’s work on compassionate leadership shows that demonstrating compassion in healthcare improves outcomes. When we do not demonstrate compassion, we see harm. If you want to know what happens when there is a lack of compassion, read about the Mid Staffs scandal.
Compassion includes self-compassion. Put your own oxygen mask on first. You cannot help others if you do not look after yourself.
Compassion consists of paying attention to, understanding, empathising with and helping others. This is crucial is when dealing with poor performance and when holding people to account. If you are a leader and do not know how to deal with these things in a compassionate way, it’s time to learn.
Compassion and niceness are not the same. Yes, a lot of the time being nice is part of being compassionate. However, if you have a poorly performing colleague within a team you lead and you do not address this, you may be being nice but you are not being compassionate to either you, your team or the poorly performing team member.
West’s work is specific to healthcare as are many of the examples I give. However, these concepts are generalisable. Let’s turn to the world outside healthcare.
Vulnerability
Brené Brown is the world’s leading researcher into vulnerability and specifically the importance of vulnerability to leadership. The orignal goal of her research was to determine how to compartmentalise emotions such as fear and vulnerability as leaders. She now argues that you cannot be an effective leader without being vulnerable.
Vulnerability is the experience we have during times of risk, uncertainty or emotional exposure. If you are a leader, you regularly experience risk, uncertainty and emotional exposure.
For example, leaders need to create forums where team members can raise concerns about aspects of that leader’s performance. This should be tough for that leader because it involves being vulnerable. Being vulnerable then allows that leader to improve themselves, improves the relationship with the team around them and improves team performance.
On her podcast Dare to Lead, Brown has interviewed the likes of Lt. Col Mike Irwin, a graduate of and assistant professor at West Point US Military Academy and Olympic gold medallist, Abby Wambach. Both embrace what Brown advocates.
What does this mean?
Let’s face it, if you’re reading this, there’s a good chance you do not like Dominic Raab. But his strongman approach to leadership is all over the place, not least within healthcare. (Anybody who interacts with healthcare will know how frequently it lacks compassion.) Is your view of what it takes to be a leader so different from Raab’s?
I imagine Raab and those of his ilk would claim what I describe as “touchy-freely”. Given that doctors, pilots, soldiers and Olympic champions buy into these newer conceptions of leadership, we are surely past that point. Leadership is about getting the best from a team, not a single amazing individual. (Or in this case, a pretty useless one.)
Stuff about leadership worth reading/listening to/watching
Just another routine operation (video) by thinkpublic for the NHS Institute for Innovation and Improvement including Martin Bromiley
So, there obviously needs to be some form of pay restoration because, well, there aren’t enough junior doctors. That or NHS trusts really likes paying locums and hate having money.
But there are things that, whilst not panaceas, could make life a lot easier for junior doctors.
Let them get married without taking a year out
My wedding is in November. I’ll be going on holiday after that. I have no idea if I’ll be able to get the time off. Now I’m a bit older and uglier, I’m just going to tell the department I’ll have the time off.
Not infrequently, junior doctors take time away from their main training programme to do things like get married. They may delay going into specialist training to achieve this because junior doctor posts are very inflexible.
One potential solution is self-rostering. Rather than giving junior doctors a prescribed rota which they pick a slot from then try to organise swaps, they get a bespoke rota for that rotation. This could be done by a reasonably junior programmer through Excel though ideally would involve bespoke software. I know nowhere with self-rostering that is worse off as a result.
Speaking of which…
Be Flexible
Increasingly, junior doctors are looking to work less-than-full-time (LTFT). This is another reason to move to self-rostering. When people work at anywhere between 50-80% a full-time rota, using prescribed rota slots becomes absurd.
Let them sleep at night
Junior doctors should all have proper rest facilities in the hospital. It is somewhat galling that at a time where lots of admin staff can work from home, junior doctors do not have the space for a bed or at least sofa to lie down on.
Doctors are periodically killed driving home. It is not currently the responsibility of trusts to ensure their staff are fit to drive home. It should be.
Not all specialties will give junior doctors a chance to nap overnight but it should be an option. The chance of a car accident after a night shift is significantly reduced with some sleep. At least give them a sofa to sleep on.
Make assessments departmental not doctors’ responsibilities
Doctors have to complete “supervised learning events” (formerly known as workplace-based assessments). These are currently the responsibility of the junior doctor to initiate.
What they are intended to ensure is that the doctor is receiving adequate education from the department. What they test is how conscientious staff are in the department; a bad department will result in fewer assessments being completed.
Currently, there are few metrics to judge how well departments do this despite it making a significant difference to doctors’ experiences of a given department.
(I probably shouldn’t be having a go at senior doctors during a strike where they’ve been very supportive. But, you know, it’s a thing.)
Compassion works
We know and have now known for years compassion is crucial to effective healthcare. If you want to know what happens when organisations completely lack compassion, just see the likes of the Mid Staffordshire scandal and the abuse at Winterbourne View.
Indeed, compassion is most important when holding people to account, dealing with poor performance and looking after oneself (self-compassion). Most of these interventions are not very costly (with the possible exception of taxis homes after a night shift).
Trusts want a way of avoiding junior doctors going on strike and asking for more money to be paid the same as their compatriots were 15 years ago. It’s cheaper to buy a few beds and ask consultants to do paperwork in a timely fashion than it is to cancel thousands of operations.
Ordinarily, I’d be having a birthday party on 7th August. My actual birthday is during the week but I’m working (alas).
Last year, due to the various restrictions, I set up a rather amusing spreadsheet to organise my party whilst adhering to the rule of six. My birthday party was outside and was fun but ultimately obviously not as fun as having loads of people round.
Ultimately, assuming the weather stays warm, I could have my birthday party outside. Given the age groups of the vast majority of my friends and the fact they are all pretty sensible, most have been double-jabbed. Were they “pinged” by the app or found to be positive, they wouldn’t come.
Most doctors agree that the government’s approach to the lifting of lockdown restrictions is nonsensical. Around 63% of people are two weeks post-2nd vaccination but it is already clear waiting longer could lead to us genuinely having control of the virus. The prospect of returning to work tomorrow to potentially spend time caring for covid patients in level 3 PPE when it’s 30°C outside is not particularly appealing either.
The benefits to the economy appear to be somewhat limited. We don’t know yet whether businesses are going to be deleteriously affected by the “pingdemic” – where the NHS Covid app notifies you of contact with somebody testing positive for covid and thus leading to large numbers of employees having to self-isolate, rendering the business unviable.
We also don’t know whether the prospect of businesses and their employees de facto turning their apps off will mean that customers fear restaurants, pubs and clubs will become covid hotspots. Indeed, it’s something that’s probably going to stop me going to them in the near future. If government was truly serious about ensuring businesses, particularly small businesses, stay viable, more money would have been available even as restrictions were slowly lifted.
So all of this brings me to the question of should I have a birthday party. I’m not sure the risk is all that high and I don’t criticise others for making a different decision. I’ll almost certainly have a birthday party, even if it’s 6 weeks or 6 months after the day in question. But the case for lifting lockdown rules is unpopular (although admittedly 1 in 5 people think we should introduce a permanent curfew after 10pm, rather worryingly) and the medical and epidemiological evidence justifying it seems weak at best.
Suffice it to say, I will be staying home most of the summer until I’m convinced there isn’t going to be another wave which it is almost certain there will be.
Remainers, progressives, liberals, pro-vaxxers and scientists share a flaw – we follow evidence…except the evidence on how to convince people of the evidence.
My title is a quote taken (with a “liberal” change) from the opening scene of The Newsroom. The series itself is of variable quality but the monologue is typical of Aaron Sorkin’s elegant writing. Indeed, it is those sort of feelings that move us to get involved in politics.
What makes the speech effective, is the emotion which both the writing and Jeff Daniels’ delivery bring. Rhetorical techniques like contrasts, rules of three, and comparisons all abound.
But it is not, however, the logic of Will McAvoy’s case. There is a coherent argument but we cannot fool ourselves into thinking that we’re uplifted by it because of that coherent argument rather than the emotion. (Also, the argument is based on what constitutes “the greatest country in the world” and is actually a bit silly.)
Leave deserved to win
If Remainers want to see the case for the EU made, the first step is accepting that Vote Leave ran a far superior campaign. Moreover, they ran an exceptionally positive one. It might not “feel” positive to you and me but “take back control” was a simple message, repeated ad nauseam, until it was all over the media, and it made people who felt out of control feel like voting leave meant taking it back.
Vote Leave recognised that they didn’t need to convince Remainers. They needed to convince the undecided – around 42% of voters in the month prior the referendum. That we as Remainers felt Vote Leave messages around taking back control and funding the NHS were both crass and unconvincing was neither here nor there – they weren’t trying to convince us.
The best guesses we can make suggest Brits spend around 25 min a day* with the news. Note: “with” the news just means the news is on – it doesn’t mean anybody’s paying attention. Further, Remainers tend to be better educated so more likely to make up the 50% above 25 min a day. The people Leave targeted are more likely to be below 25 min a day.
In terms how much time people spend actually consuming news, it’s probably going to drop down to single figures.
Can you explain the EU in 8 seconds?
Come on. You know you’ve done it. You know you’ve shared a piece you haven’t read, based on the headline. There is a reason the front page of a newspaper, the headlines of TV and radio news, and the most prominent articles in online news are the most eye-catching. News outlets are in the business of selling and that’s the best way to sell.
Arguments about the EU are won and lost in headlines because this is the place that the vast majority of people consume their news. Vote Leave figured this out – it didn’t matter that an erudite Guardian columnist had waxed lyrical and delivered a devastating blow to the Leave case for closing the borders on page 24 in the Comment Is Free section. Those columnists are designed to get you and me to pick up a copy of the Guardian, not to win an election.
And even then, there are myriad other things in the news, competing for consumer attention let alone the things that make up the other 23 hours and 35 minutes of the day. If the headline you want comes on on the radio but the kids are dicking about in the back of the car, that parent is going to be distracted and miss the story.
So my best guess is we have seconds to make these arguments.
Emotions matter
Let’s be clear – Remainers are neither brighter nor cleverer than Leavers. Remainers voted on equally emotional grounds to Leavers. We like the idea of the EU, of working together with others, of a multicultural society, of being able to experience new things with minimal hassle, of our children and our children’s children being part of multilingual and diverse families stretching across a continent with shared values and ideals.
Perhaps you genuinely believe the reason you voted Remain was because you made a rational and logical decision. Perhaps you assessed all the facts, all the competing factors and all the nuances of European geopolitics and the historical context of Britain’s relationship with Europe. Perhaps you succeeded when people who have PhDs and professorships have examined these arguments and these stories and have spent years and lifetimes trying get to grips with these ideas. After all, you spent 6 months reading the Guardian and even the FT semi-regularly on the train to work.
Or perhaps your decision was just as emotional as everybody else’s.
Until you can come to terms with the fact that you voted based on emotion, it’s very difficult to effectively contribute to a political change. That you voted with emotion doesn’t meant that you’re wrong about what you’re voting for. (I absolutely believe there is a coherent logical argument to remain in the EU over and above that to leave.) And it is that emotion that drives political activists to try and make the changes they want to see. But we have to acknowledge that emotion.
What can you actually do?
1. Delete the retweet
Repeat good ideas, not bad ones. George Lakoff – the author of Don’t Think Of An Elephant – argues than when dealing with a lie, think about the truth that the lie is trying to cover up.
Negating a lie, amplifies that lie. Our brains struggle to process negatives. The recent coverage of the Education Select Committee report on the failures around white working class kids talks about the term “white privilege”. We could enter into a long-winded debate about what “white privilege” means. Or we could just point out that the report shows government failing every child outside of London and that most of those happen to be white.
Moreover, social media algorithms amplify the things you retweet or share. But even the screenshot – designed to avoid this – still amplifies lies.
Amplify the truth, not the lie.
2. Joining a political party is a waste of time; you have to do stuff
Joining a political party just so you can have a membership card is pointless. It’s £12/year to join the Lib Dems – this isn’t that big a financial boon for the party. Go to meetings, deliver leaflets, knock on doors. But don’t be under any illusion. Whilst the goals may be beneficent, the people in it are often not.
All the politics of the office are equally applicable to the politics of politics. I have been criticised and my partner had false accusations of criminal behaviour levelled at her by a senior local party figure (since retracted) because I posted that I thought Liberal Democrats shouldn’t be Facebook friends with Chris Rennard, a man who dodged a proper investigation into “credible evidence” of sexual harassment because the disciplinary process at the time was unfit for purpose. My subsequent experience of the party’s new disciplinary process (around the accusations levelled at my partner) has filled me with no confidence in it.
(I’m still not really sure why anybody thinks it’s super important to be Facebook friends with the guy but it’s apparently very important to some people.)
I’m not currently active – in part because of the above – but this is one of the few ways one can be truly effective in effecting political change. I’m not saying don’t join, I’m just saying don’t expect it to be a perfect or even necessarily a good experience. And the Liberal Democrats are generally considered one of the nicer parties internally.
And ultimately…equal marriage, shared parental leave and the rise in personal allowance would never have happened without the Lib Dems.
3. Your “sick burn” just sets everything on fire
Insults polarise debate (although admittedly, it got you to read this far down). I get that it feels good to post the meme about how crazy anti-vaxxers are but ultimately, you’re not going to convince anybody to vaccinate their kids by calling them an idiot. Indeed, insults will force anti-vaxxers to entrench their views ie insulting anti-vaxxers probably decreases the rate of vaccination.
Making things seem normal (so the profile pic saying you’ve been vaccinated) does help though. It’s easier to consider something safe if you see others around you doing it too.
It’s not always possible and I’m not here to be the tone police. Occasionally, it is necessary to make an overt political statement. But most of the time on your Facebook profile, posting clever memes about how dumb Brexiteers are is just going to entrench Brexiteer positions even more. You’re making everybody’s job harder.
Too late for some
Clearly, we aren’t going to rejoin and I’m ambivalent about “rejoin” anyway which probably puts me in a minority amongst passionate Remainers. But if you want to make the broad case for a close relationship with the EU, the 100-comment doom-thread on your personal profile isn’t going to cut it.
It needs to be simple, emotional, repetitive.
References
I haven’t specifically referenced stuff as I’ve gone along but this a reading list for people who want to learn more about political communication.
Don’t Think of an Elephant: Know Your Values and Frame the Debate by George Lakoff
The Science of Marketing: For Business and Politics by Richard Maxwell (conflict of interest, Rich is a mate)
The first two are books, the last is a course I did about 4 years ago. It’s free and run by Delft University and it goes through step-by-step the concept of framing and how political communication works.
*Rasmus Kleis Nielsen actually puts forward an estimate of 25-74 minutes. However, he states that the 74 minutes is based of self-reporting and there is evidence that self-reporting multiplies actual TV watching time by around 3 times (which is how he came to the low estimate). That makes the most sense in my mind so I’ve gone with low estimate as the more accurate one. But even then, I think the logic still holds.
Google Images search results for “flatten the curve” at 14:01 UTC 1/5/2020
As the scope of covid-19 (coronavirus disease 2019) became apparent over the course of March, news outlets, health organisations, and scientists and medics started to advocate measures to “flatten the curve”. The term was too abstract for popular use and was rightly replaced by the simpler #StayHomeSaveLives.
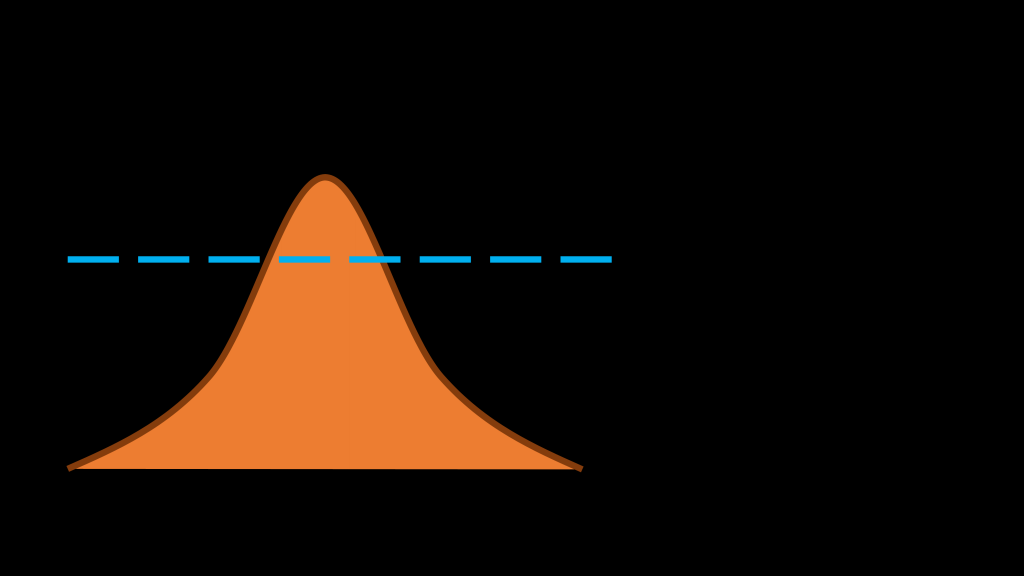
The case for this was relatively simple. Imagine a curve representing the number of people with coronavirus over time. Initially, the numbers will be very small but increase as the virus spreads. People get better or die and so eventually the number of people infected drops. The curve would look like this:
Time moves from left to right. The orange curve represents the number infected with coronavirus.The blue line represents critical care capacity. You’ll note the orange curve goes above the blue line.
Now, that statistic is a little misleading. There is a lag between contracting the virus and developing symptoms (thought to be around 2 days) and then requiring critical care (my anecdotal experience is this is at around 10 days of symptoms). This also doesn’t take into account people who have got better. That is to say, the curve for critical care admissions will be around a week and a half behind the curve for total confirmed covid cases.
In China, around 5% required critical care. At the start of April, the World Health Organisation estimated around 10% would require critical care. There are also debates around what constitutes critical care in different countries – we’ll get to that.
There are three ways to deal with the crisis:
Raise the capacity of critical care (raise the blue line)
Reduce the speed of spread (“flatten the curve”)
Treat or cure coronavirus (reduce the area under the curve)
In Northern Italy and Wuhan, hospitals had little warning of the impending crisis. As such, their hospitals were in no way prepared for the onslaught. They had no way to raise the blue line or flatten the curve prior and were overwhelmed.
As such, patients requiring critical care admission would likely have died or will diebecause they received what would normally be considered suboptimal care.
Level 1 care in the UK is normal ward-based care. (Sometimes, this is referred to as level 0 with level 1 care being some level of extra monitoring.)
Level 2 care (the High Dependency Unit) involves nurse:patient ratios of 1:2 and typically involves single-organ support – either non-invasive ventilation or vasopressors/intropes (drugs to raise blood pressure/increase heart contractility).
Level 3 care (the Intensive Care Unit) has nurse:patient ratios of 1:1. It will either involve support of 2 or more organs or invasive ventilation or renal replacement therapy. Invasive ventilation means initially anaesthetising a patient so a breathing tube can be inserted and then providing sufficient sedation such that the patient can be attached to a ventilator and keep the tube in. Renal replacement therapy is a broad term which includes the intermittent haemodialysis that most patients who visit dialysis units as outpatients receive. Most ICUs perform continuous renal replacement therapy ie the patient is attached the whole time.
“Critical care” is a catch-all term for level 2 and level 3 care. In some hospitals, HDU and ICU will be amalgamated – the number of level 2 and 3 beds will be determined by nursing staff availability. In others, HDU and ICU will be separate. This may be next to each other and covered by the same staff or completely physically separate. There are often specialist HDUs and ICUs (cardiac and neuro ICUs are the most common in big central hospitals but separating surgical and medical HDUs is also common).
The point of all this? Northern Italy and Wuhan critical care staff would have been trying to deliver these complex and specialist therapies all across the hospital without the requisite staff or equipment.
In the UK, we’ve had warning and have been able to prepare. The experience is not uniform across the country. London has been hit particularly hard. The reasons for this will need investigation in the future but it is perhaps unsurprising that a dense city with large numbers of international inhabitants, multiple airports, and an efficient public transport network has seen a faster spread of the disease.
Elective operations across the country have been cancelled. Critical care units have been reorganised or moved so they can provide a higher number of ventilated beds. This has meant staff not usually involved with the care of ventilated patients (and in many cases, having never administered IV drugs) being allocated to these patients, often from places like operating theatres. But crucially, Britain has had time to prepare – in Italy and China these changes would have happened on the fly as staff struggled to keep these patients alive around them.
It’s worth noting that “critical care” in some countries merely means that they are getting some extra monitoring. One consultant from Germany remarked this may be nurse:patient ratios of 1:4 – hardly what we would consider critical care.
Flattening the curve
In the above graph, the green line represents what happens if we’re socially distanced. The line never goes above critical care capacity. As such, although people will still die of coronavirus, these are patients who cannot be saved by what we have to offer in modern medicine.
Let’s say you have a small critical care department who have optimised such that they have 10 critical care beds which can provide ventilation to all and renal replacement therapy to some. With the orange curve, let’s say you see 20 patients requiring on average, ten days of ventilation at the same time.
This will overwhelm your critical care unit and people will suffer harm. If however, it’s the green curve and let’s say the 20 patients are now staggered over a period of a month, it might be that at most, you are caring for 10 patients but at different times. It means your department can cope without the need for significant extra resources.
Big curves v flat curves
There has been much criticism of Boris Johnson’s approach to the government whereas Jacinda Ardern, the New Zealand Prime Minister, has received a great deal of praise for her management of the virus.
Ardern locked down much more quickly. New Zealand has effectively stopped its spread in the community. By contrast, the UK faces controversy over its failure to include care home deaths in its statistics and a rise therein during the crisis.
The truth is as ever more complicated. The question is not “have we stopped the spread of coronavirus?” – that is, until we develop a vaccine or cure, impossible. A large proportion of the country will be infected. If the currently weak suggestions that reinfection are a risk are true, then the story is more complex still and it is likely an even larger proportion of the country will be infected (plus those who are reinfected), regardless of what we do.
It isn’t even as simple as the number of folks infected. It’s the number person-days that people are infected and that is measured, crudely, with “area under the curve” ie if one person has the infection for 4 days, that’s the same as two people having it for 2 days or four people having it for 1 day. The bigger the curve (taking into account both height and breadth ie “area under the curve”), the greater the disease burden. Currently, we seem to treat flattening the curve as the same as reducing the area under the curve.
Social distancing will delay you getting the disease but it won’t in and of itself stop you getting it. What it will do is mean that if you or your family require critical care, they’re more likely to survive as a result.
Diminishing returns
Of course, what if we have massively overreacted? Does it even matter? After all, better safe than sorry, right?
Well, not quite. Patients who don’t have coronavirus are suffering. Very early on, I saw one patient nearly lose a limb because of overly protective advice from 111. Cancer operations and treatments (such as chemotherapy) are being delayed. Routine outpatients will still need catching up. All of this will delay diagnosis and treatment of illness, much of it potentially life-limiting.
There is a wider impact on mental and physical health. Children will have to catch up with their education. Jobs will be lost – businesses have already gone under – and this will have a further major impact on mental and physical health. We know recessions cause a rise in suicide rates and probably a more general increase in mortality.
Regardless of your opinion of Boris Johnson, the decision of when and how to reopen the economy is tough. Certainly where I work, we are coping well with the crisis suggesting the measures taken by our trust are about right (though this is not true across the whole country).
The difficulty is, the results of any change in policy on lockdown will not been seen on critical care units for 1-2 weeks. And even if that change at that point is reversed, there may still be ongoing increases in infection rates and concomitant critical care admission for further weeks following that change with a potential to overwhelm.
Equipment
The shortages in equipment have been widespread. GTech produced a “ventilator”, entirely unsuitable for use with covid patients (and a rather expensive way to provide humour for the doctors on critical care where I work). Elon Musk’s “ventilator” turned out to be non-invasive ventilators which is rather like me saying I’ve produced a new electric car and showing them my ebike.
Currently, the most prominent shortages are those of personal protective equipment (PPE). PPE comes in different forms and different patient groups require different levels of PPE.
I work on a critical care unit completely dedicated to covid but I do have to go and review patients on the ward. Why is there so much confusion regarding this?
Aerosol-generating procedures
Aerosols are particles ≤ 5 micrometres (five-thousandths of a millimetre). Droplets are > 5 micrometres.
Only certain procedures generate aerosols; these are largely procedures involving instrumentation of the airway. Intubation – the insertion of a breathing tube in the windpipe below the vocal cords – is probably the most relevant. But equally, patients on ICU on a ventilator, will not infrequently have their ventilator disconnected which will then generate aerosols.
There is some debate about it but currently, non-invasive ventilation (a mask or hood that provide ventilatory support in an awake patient) and high-flow nasal oxygen are also classified as aerosol-generating.
As such, our entire ICU is classified as an area at high-risk of aerosol generation and therefore level 3 PPE is required. This means when I go in, I don: a pair of undergloves, a long-sleeve surgical gown, a long second pair of gloves taped to the gown, an FFP3 mask, a theatre hat and a visor. I then don an apron and a third pair of gloves which I swap between patients. I wash the second, middle pair of gloves between patients as though I’m washing my hands.
However, if you’re not doing a aerosol-generating procedure, the issue is droplets.
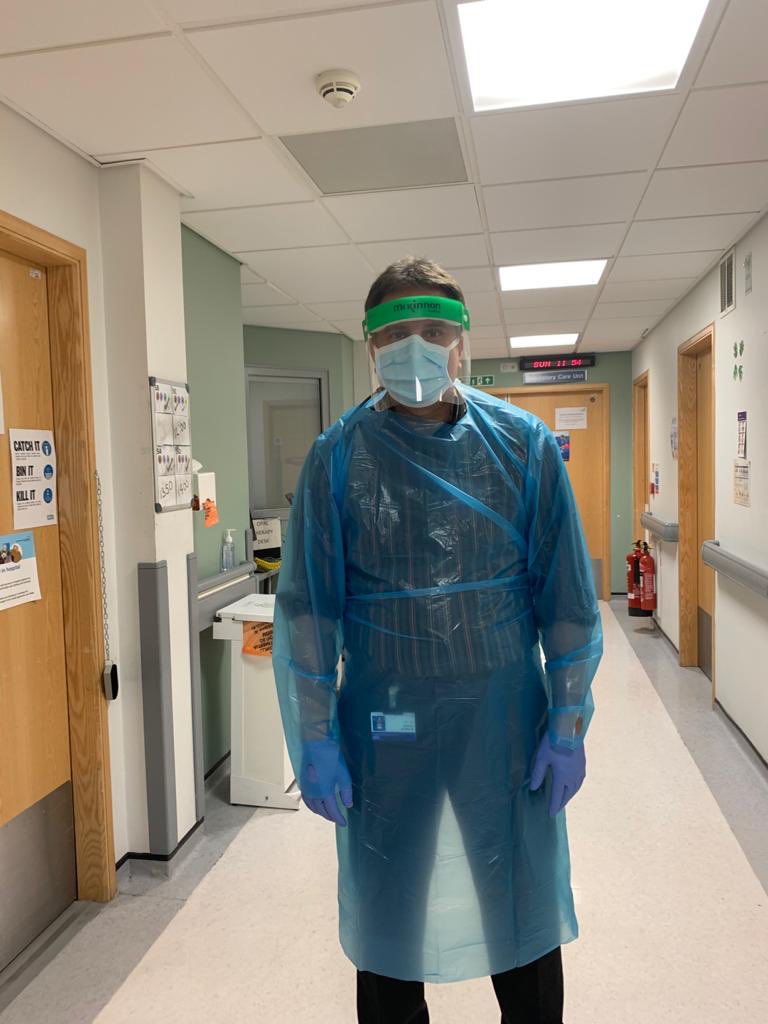
I got into a Twitter spat with a fellow Lib Dem who shared the picture on the right, claiming this was inadequate PPE. It was annoying as it is actually perfectly adequate PPE for dealing with low risk patients (note the link is for current PPE requirements but they were adequate at the time).
More irritatingly, I’d gone to see patients in exactly that PPE. I’m very happy to see patients in just an apron and where required, not even the plastic gown pictured.
This isn’t because I’m well-hard (though I do suspect I have had covid despite my negative swab). There is potential to contaminate yourself whilst removing the PPE – indeed, this is probably the most high-risk point of the whole procedure.
If I am seeing a patient where there is only risk of droplet infection, I am quite happy to review that patient with only apron, gloves, surgical mask and face protection. I’ll abide by whatever PPE instructions that particular ward is using. The key thing is still, in these cases washing, washing, washing hands. I worry that folks see the TV and think everybody should be in full ICU-style PPE when it isn’t really necessary and only works if, like we have on ICU, you have designated donning and doffing areas with buddies to help you do this.
So the government has got it all right then?
Well, no.
The anonymity of those on SAGE (Scientific Advisory Group for Emergencies) is concerning (although some its members do identify themselves). It is all hardly in keeping with the general feeling science should be transparent. One would think Dominic Cummings and Ben Warner, both political appointees, have no place on it.
The failure of the government to join the EU in its bulk-buying of PPE too deserves criticism. Professor John Ashton, Former President of the Faculty of Public Health, was highly critical of the government’s failure to stockpile PPE for a pandemic and it appears rightly so.
All that said – it’s going to be months if not years before we can determine whose approach to coronavirus has been more effective. It genuinely isn’t clear if the over 100 NHS workers who have died of covid, died because of inadequate PPE. Ardern’s approach in New Zealand may simply be delaying the inevitable whilst harming her economy and her country for little gain. Doing so whilst people die from the detrimental effects on the wider determinants of health caused by the lockdown is no victory.
Simply looking at covid deaths tells us little about the effect of lockdown. We need to a look at all-cause mortality for this period and for some time following to determine exactly what the consequences of covid are and what approach was best.
As a seasoned TV watcher, sitting and smashing out hours in front of the box during my free time is pretty standard for me. However, I appreciate that watching The Shield or Rick and Morty, whilst both very good, aren’t exactly uplifting shows and indeed aren’t everybody’s cup of tea.
This is a list of what I consider high quality television without the seemingly modern staple of being “dark and gritty”. (And I love dark and gritty.)
(Note – these are not in any particularly order. Mainly because I couldn’t be bothered.)
1. The West Wing
7 seasons, 156 episodes (1999-2006)
A lot of people will have already seen this show and it is part of the pantheon of television in the late 1990s and early 2000s that started an enormous leap in quality across the board. I’m not sure it’s possible to write 4 22-episode seasons without the aid of recreational drugs but his dialogue-filled episodes can be watched multiple times over.
“But people just don’t speak like that” is a legitimate criticism. Women are often awfully written in his shows and there are plenty of cringeworthy moments (no Charlie, it is not OK to suggest you’ll watch CJ getting changed). So it’s a not a perfect show. But seasons 6 and 7 – after Sorkin’s tenure – pick up. And even season 5, its worst season, is still head and shoulders above most other TV.
All that said, the positivity about politics on both sides of aisle can be a refreshing escape from today’s partisanship. If you’ve never seen it, now you’re stuck at home, this is a show that will make you feel better about politicians, even if only fictional ones.
(And no – it is not a prerequisite to know lots about politics.)
2. The Good Place
4 seasons, 56 episodes (2016-2020)
The premise of this show is simple: Eleanor Shellstrop is dead and has accidentally been sent to heaven, despite the fact she knows she shouldn’t be there.
The show is funny whilst exploring philosophical thought experiments about the nature of good and evil. The characters are likeable but at the same time morons in their own right, making them all the more relatable.
Visually, the show is a tonic to the plethora of grey shows with grey backgrounds that look grey (and feel dark and gritty…and grey). It adds to the feeling of it generally being upbeat.
Although the show does have dips in quality, and it is far from perfect, if you want something that will make you laugh whilst also making you think, this is the one for you.
3. The Marvelous Mrs Maisel
3 seasons, 26 episodes (2017- )
I’m somewhat surprised this show isn’t being talked about more. Midge Maisel is a 1960s housewife who, following her divorce, becomes a comedian.
I guess this hits home a little as I’ve tried but given up stand-up and have an idea of how difficult it must be for a jobbing comic. Often shows like this can come across as unnecessarily twee or descend into farce and so lose their realistic edge that grounds them and makes them relatable.
Amy Sherman-Palladino does quite the job of ensuring this doesn’t happen. I couldn’t tell you why or how but even the most cynical amongst you (and let’s face it – I’m quite the cynic) will find enough in this to make clicking “play next” very difficult to stop. Amazon Prime is pumping out some excellent television and this is certainly part of it.
4. Borgen
3 series, 10 episodes (2010-2013)
Look – it’s not Danish West Wing and I sort of wish people would stop calling it that. The West Wing very clearly sacrifices telling personal stories about its characters in order to tell its political ones. Borgen is very much the personal stories of politicians interspersed with political ones.
I don’t think it’s as good as the American comparator but that doesn’t mean it’s not worth watching. OK, it’s a bit of a fantasy that the Danish equivalent of the Liberal Democrats come smashing through the centre to dominate politics and win the country’s premiership but it’s a fun and engaging fantasy nonetheless.
Much like The West Wing, there are some extremely dark moments to the show and it’s not pure positivity (are there any good shows that are?). But it is does a good job of selling politicians as people, largely trying to do their best within the limits of being elected.
5. Parks and Recreation
7 seasons, 125 episodes (2009-2015)
Fair warning – the first season is quite bad. Not awful but quite bad. They tried to do something I think more akin to The Office by having things be awkward and weird. When they switched to trying to tell more positive stories about the sort of folk who work in American local government and their attempts at fulfilling their hopes and dreams, the show found much surer and more effective footing.
Leslie Knope (Amy Poehler) is the Deputy Head of the Parks and Recreation department in her fictional hometown of Pawnee, Illnois and is a passionate, if overzealous believer in the power of government to do good. Her boss, Ron Swanson (played by the brilliant Nick Offerman), is her conservative anti-government libertarian boss who opposes government doing anything and does as little in his job as possible.
Surrounded by a wonderfully quirky ensemble cast and excellent recurring characters, it’s the third show on this list that paints a picture of positive politics but in a very different way to The West Wing and Borgen. No matter whether you’re interested in politics or not, it is well worth a watch.
Yesterday morning, I woke up to the wonderful news that Jane Dodds is now MP for Brecon and Radnorshire, bringing the Liberal Democrats parliamentary party to a nice, prime 13.
However, as this blog post from the chair of LGBT+ Lib Dems explains, despite the news being wonderful, there are reasons to be less cheerful. It’s short and worth reading but amongst various things, she highlights that in a marginally Leave-voting constituency (52-48), explicitly Leave parties (the Brexit Party, Tories and UKIP) outperformed the only explicitly Remain party (the Lib Dems with Plaid Cymru and Greens admirably standing down).
At the Humanists UK Convention a few weeks back, I was lucky enough to attend a lecture from Professor John Curtice of “my 2015 and 2017 exit polls are better than yours” fame. In the last few months, Remainers point to polls now favouring them, were a People’s Vote to happen immediately.
However, Professor Curtice adds a strong note of caution. Break down the numbers and equal minorities – around 8% – of Remain and Leave voters changed their minds. So why is Remain now winning? The Did Not Vote’s are 50% Remain, 25% Leave, 25% Don’t Know/Would Not Vote (source).
Professor Curtice argued that if a People’s Vote were held tomorrow Remain would rely on turnout of those least likely to vote.
Reasons to be more cheerful*
A week is a long time in politics and the 15 months since Patrick Stewart and a number of pro-Remain politicians launched the People’s Vote campaign have been longer still. We have a new Prime Minister with a smaller majority and the entirely new Brexit Party pushing the Tories further towards hard Brexit.
When it started, the notion that a People’s Vote would even be seriously discussed was fanciful. But fanciful ideas are largely ignored by Prime Ministers; when Theresa May started having to openly attack the idea of and declare that she did not support a People’s Vote, the campaign was working. The notion of a referendum on her deal was if not widely accepted at least a mainstream one.
The campaign has been persistent and tireless. Those involved in it deserve much credit and indeed without it, it’s entirely possible we would have left with either an appalling deal or indeed no deal at all as hard Brexiteers within and without the Tory party held its feet to the fire.
The failure of fact-checking
Probably the most prominent non-politician of the People’s Vote campaign is Femi Oluwole. I follow him on Twitter and whilst he works incredibly hard talking to folks all over the country about Brexit (including some of the staunchest Brexiteers), it’s become clear that a large proportion of what he does is fact-checking.
Clearly, doing some fact-checking is important. But Stronger In lost because it spent so much time repeating the lies of the Leave campaign. Sure, the media deserves blame too as too often it uncritically repeated Leave’s lies but the naivety of those leading the Remain campaign is now obvious to all. You cannot win a political campaign by simply quoting sound statistics.
There has been little to demonstrate that People’s Vote has changed that tactic. Indeed, a further point Professor Curtice made is that people have become more polarised over Brexit, not less. The middle ground of people who supported some sort of deal with the EU has become smaller with people filtering to both extremes.
This means that a People’s Vote would arguably be even harder to win. Rather than preaching to the uninitiated, we would now be trying to convert a relatively small and relatively difficult to target group of folks who either didn’t vote previously or have changed their mind.
(Also, thanks Led By Donkeys but uncritically repeating Leave politicians lies in Leave areas is going to do the square root of jack to change people’s minds. It just reinforces whatever your pre-exisiting bias is. Stop it.)
Why is the framing so hard?
I think one of the reasons liberals/progressives/centrists/Remainers/#FBPEers find it so hard is that the obvious benefits are only apparent to those who have already bought in. Discussing the EU as a peace project sounds nice but nobody seriously believes that a European war is going to happen who isn’t already voting Remain.
After over two decades of both Conservatives and indeed New Labour doing little to combat the rhetoric, the idea that immigration is harmful persists across large swathes of the country. Reversing that is hard. And #ProjectFear rather successfully put paid to the idea that “it’s the economy stupid” was going to be effective amongst the poorer Leave voters who had seen pay cuts, job losses and drops in their standards of living due to a recession the likes of which were allegedly consigned to history. (Though I note that most Leave voters were middle-class Tories.)
I don’t have any grand solution. I suspect the answer has to be figuring out a way of selling immigration as a good thing, as a financially beneficial thing and as a thing this country should want to stand up for. And to be honest, it’s not just about Brexit but about what we want the country to look like for the next 50-100 years. That fight is now but everybody is too busy looking at the trees made from satirical memes about lying red buses to see the woods of a political discourse that will define this country for generations to come.
*I have never actually listened to the Ed Miliband podacst Reasons To Be Cheerful.
Last week, I joked on Facebook that when I attended the Saturday Leeds leadership hustings (168 hours early), it would be helpful if one candidate could steal a baby or kick a puppy. It would make it much easier to choose between them, though I’ll not say which way my vote would have swung.
I have now seen them in person in Leeds and subsequently watched the North West hustings on YouTube. The criticism that they are too similar does not do the contest justice; the differences are there if you look beneath the surface.
There is no doubt that Ed Davey’s experience and knowledge are impressive. He rightly – both in terms of his audience and as a prospective government agenda – leant heavily on his green credentials. His explanation of how 15% of greenhouse emissions come from organisations which go through London, his wider emphasis on a green economy, and his advocacy for renewable energy as a source of jobs and investment for the future all served him well.
From his support for LGBT+ rights, pushing for support staff in the climate department to receive a living wage, to freeing a constituent from Guantanamo Bay, he is more than just the green candidate. Despite some (I think unjustified) criticism of his approach to fracking in coalition, his liberal and indeed Liberal credentials are a struggle to question. I believe he would be an excellent leader.
So why Jo?
Individually, many of Jo’s policies are for a Liberal Democrat perhaps unremarkable. She would rather spend money on early years education than on free University tuition fees. She believes companies should have to produce data on employee job satisfaction and social good. She has argued that automation will have profound consequences for our economy and we need to protect those that are most vulnerable to it.
When politicians – or indeed Jo – talk about transforming the economy, it is tempting to stop listening. On its own, it is a phrase devoid of meaning.
But when you start to take “transforming the economy”, putting “people and planet first” and add it to her rhetoric particularly on technology, you start to see her broader political vision. The manner in which she has discussed technology suggests that of the two, she better understands that it will not be enough to make renewable energy the new industry.
From Uber drivers to accountants, actuaries to Amazon delivery drivers, the problems of automation must be front and centre of that economic transformation. We need a plan for when the skill sets of millions are rendered obsolete by enough RAM and, yes, maybe even robots.
Jo has touched on universal basic income but like any solution she admits that it is neither a panacea nor without potential harms. I can’t tell you exactly why in her leaflet she mentioned her programming on a ZX Spectrum 48K, but when put in context of her rhetoric around technology, it adds to the sense that she has keener grasp of what will potentially be a more potent threat to our economic norms than even Brexit. You only have to look at the intergenerational poverty wrought across Wales, the East Midlands and the North by Thatcherism’s failure – either through neglect or malice, pick your poison – to properly reskill an entire generation of manual labourers.
Who has the best “-ism”?
From Ed, I get the sense of a man with an in-depth understanding of the ramifications of policy and how to best optimise them in every area. But I don’t have a sense of what “Daveyism” might one day look like. I know that it would involve investing in renewables and taking on the climate emergency. I know it would involve doing our best to protect individual liberty. And I know it would be an approach of internationalism. But it is a collection of liberal policies not seemingly tied together other than being individually good ideas. And that is, rightly or wrongly, what I took from Ed’s hustings performances.
With Jo, I see the start of a broader political vision. I can see what “Swinsonism” might begin to look like. Her argument is that we need to move away from old ideas that put GDP above all else. Couple that with the obstacles and opportunities she sees in the technological revolution. It could be the key to solving the climate emergency by transforming industries such as food and transport, both major contributors to CO2 production, but also needs to ensure that drivers of lorries, taxis and delivery are not left unemployed by drones and driverless cars.
Thatcherism was the idea that supply-side, free market economics would generate wealth such that gaps in inequality mattered less than absolute rises in living standards. Blairism advocated flourishing free markets with sufficient tax to build a proper welfare state. Swinsonism believes old economic models are obsolete and technology will render them more so: whatever our solutions, all roads must lead to empowerment of the individual whilst protecting the planet.
An election is seldom fought on the same terms as the previous one. In 2017, nobody mentioned a Labour-SNP coalition. In 2015, few agreed with Nick. In 2010, a global recession had eclipsed the war in Iraq.
In a future where Ed Davey becomes Prime Minister, I might know what policies he intends to put in place. I don’t know what the underlying philosophy behind them is and I can’t instantiate what he would do in the face of change. Jo Swinson advocates ensuring that whatever the change, empowerment of the individual has to be the metric used to make every decision.
No, Prime Minister
There are two issues with the above. Firstly, neither Jo nor Ed is likely to be Prime Minister. Sure, the Tories and Labour may collapse but first-past-the-post means it is still more than likely the red or blue team will be in Number 10 after the next election. It would surely be better to judge them on their campaigning ability rather than some hypothetical political philosophy.
Secondly, I might be wrong about Jo. Politicians tend to fail more than they succeed. Both Ed and Jo were part of a coalition government that whilst successful in many ways (pupil premium, shared parent leave, same-gender marriage), irreparably damaged many people and our party too.
Nick Clegg may have been the darling of British politics in 2010 but it’s clear now that he made by his own admission many, many mistakes that would eventually be his undoing. And anyway, perhaps I’m reading too much into an equally disparate collection of Swinson policies whilst ignoring what guides the Davey political compass.
All that said, I think there is little to choose between them in campaigning terms (though I do think Jo is a slightly better media performer and public speaker) nor on their CVs. As such, I am left only with what they might want to do in power.
With Ed Davey, I feel I know what he would want to achieve in his first 10 weeks. With Jo Swinson, I think I might be able to figure out what she would do if she had 10 years.
tl;dr – F1 and F2 are Foundation doctors (years 1 and 2) just out of medical school. CT1-3 or ST1-9 represent the number of years a doctor has been in specialty training (you need to complete the Foundation Programme to enter specialty training).
Recently, I posted on Facebook trying to find out if anybody not in healthcare understood the grading system doctors used. The answer was “no”. So I’ve created a flow chart which is too small but I’m hoping when you click on it and enlarge it, it will be fine.
The American system is relatively simple – intern (year 1 doctor), resident (doctor in specialist training), attending (doctor who has completed specialist training). American medical school is longer and their postgraduate training programmes shorter than in the UK. Whether this better or worse is debatable but intern-resident-attending is a fairly simple structure.
Assuming you took no extra time out, the old British system went like this:
Year 1: Junior House Officer (JHO) (aka Pre-registration house officer or PRHO)
Year 2-3: Senior House Officer (SHO)
Year 4-7: Specialist Registrar (SpR)
Consultant
SHOs often flitted between different jobs and some doctors spent many years doing a variety of different thing. Once they decided on the specialty (NB: specialty not speciality – it’s not a dish) they wished to pursue, they would apply for SpR jobs using their CVs from their previous SHO jobs.
This system was introduced following the 1993 Calman Report which led to the 1996 Calman Reforms. These endeavoured to provide more structured training. Prior to this, there was a registrar (note, no specialist)-senior registrar (SR) divide.
Brave new world
The route you take depends on the specialty you enter.
Why don’t you build me up, buttercup…
Modernising Medical Careers (MMC) introduced the Foundation Programme and Specialty Training in 2007. The grades now go like this:
Years 1-2: The Foundation Programme
Foundation Year 1 (F1/FY1) – equivalent to JHO
Foundation Year 2 (F2/FY2) – equivalent to a year 1 SHO
Years 3-6/7/8/9: Specialty Training (length depends on specialty)
Specialty Trainee 1 (ST1) – Year 2 SHO
Specialty Trainee 2 (ST2) – Year 3 SHO
Specialty Trainee 3 (ST3) – Year 1 SpR
Specialty Trainee 4-6/7/8/9 (ST4-ST6/7/8/9) – Year 2-4/5/6/7 SpR
Consultant
The old JHO jobs consisted of 6 months in a medical specialty (respiratory, renal, gastroenterology etc.) and 6 in surgery (general surgery, cardiac, vascular etc.). Doctors would then apply for SHO jobs which again usually lasted around 6-12 months. After two years or more, usually you could go on to apply for a SpR job (or “number” meaning National Training Number).
The new system did away with this. You did two years of the Foundation Programme consisting of usually 3 x 4 month specialties per year. In F1, you had to do 1 medical and 1 surgical specialty but it also allowed exposure to areas such as GP, psychiatry, radiology, pathology.
It also largely avoided the situation of SHOs being “too experienced” and being unable to enter an SpR programme. An interview panel might look unfavourably on somebody who had done 4 years of SHO jobs without getting an SpR number; they might infer problems that had prevented them from securing a more senior job earlier.
It’s actually relatively simple – F1 is a year 1 doctor. F2 is year 2 doctor. ST1 is 1 year after foundation. ST6 is a 6 years after foundation. The number tells you how many years they have been in specialty training. However, confusingly, the generic term for those in specialty training was Specialty Registrar (StR) (as opposed to Specialist Registrar or SpR).
The idea was that once you’d applied for specialty training, you had a clear path achieving your Certificate of Completion of Training (CCT) which allows you to practise as a consultant.
…just to let me down and mess me around?
MMC was initially a disaster. It led to a bizarre situation where doctors in the old SpR programme had to apply for their own jobs in the new StR programme. Many ended up having to drop down grades because they failed to get jobs they had been doing for years.
Applications for specialty training began halfway through the F2 year. F2s had to choose what specialty they wanted to pursue after 18 months of practising medicine. In recent years, it has led to the “F3” year where doctors leave the Foundation Programme and use it to travel abroad or locum prior to starting specialty training.
The old SHO system gave doctors time to experience different specialties. Further, it meant that doctors often had broader experiences. Medical doctors who had done orthopaedics, vascular surgeons who had done neurosurgery, GPs who had done rheumatology – all of that experience was lost.
What the new system gives you in stability, it takes away in flexibility.
To confuse matters further, an Specialty Registrar Year 1 (ST1) is not the equivalent of an Specialist Registrar Year 1 (it’s a year 2 SHO in the old system). It’s why most people avoid the term “Specialty Registrar”. Colloquially, when people mean “registrar” or “reg” or “SpR”, they mean somebody who is ST3 or above in their specific specialty.
The core issue
So, it’s not even as simple as above. There are 6 “core” training programmes of which I am aware. Instead of doing ST1 & 2, you do CT1-3 and then enter a specialist training programme at ST3. (Yes, confusingly, you might go from CT3 to ST3.)
Core Medical Training – for most internal medical specialties (including acute internal medicine) and intensive care
Core Surgical Training – for most surgical specialties
Core Anaesthetics Training – for anaesthetics and/or intensive care
Acute Care Common Stem – for 4 acute specialties: anaesthetics, intensive care, emergency medicine and acute internal medicine
Core Psychiatry Training – for psych specialties
Broad Based Training – for GP, paeds, psychiatry and most medical specialties
In terms of experience in your field CT v ST makes very little difference. However, in an ST programme, it’s run-through – there is no application between ST2 and ST3 (generally). With the core programmes (called uncoupled training), you have to apply for an ST3/4 job once you’ve completed you core training.
You’ll see that you can get into anaesthetics, internal medicine, acute internal medicine, intensive care and psychiatry through two routes. You can also get into paediatrics by entering a dedicated programme as well as broad based training.
General Practice
GPs, the folks with the hardest jobs in medicine, are as ever much more sensible.
Year 1-2: the Foundation Programme (as above)
Year 3-5: General Practice Specialty Training (GPST)
Year 3-4: mixture of GP and hospital-based practice
Year 5: all GP
GP Principal (a fully trained GP)
Foundation – Specialist Training – GP…that is pretty simple.
Why are we still talking about SHOs?
The term “JHO” has completely disappeared. On the ward, folks refer to “the F1”. However, the old SHO in modern terminology might be:
an F2
a CT1-3
an ST1-2
a GPST in hospital
Rotas are still split: F1 (fka JHO)-SHO-SpR-Consultant in most places or just SHO-SpR-Consultant in something like anaesthetics. Theoretically, this should be:
F1
Junior Grade (SHO)
Middle Grade (SpR or equivalent)
Senior Grade (Consultant)
Within a rota, most folks have an understanding of the minimal level of competence expected of an SHO/junior grade or a middle grade/SpR in a given specialty. The issue previously had been that a day 1 F2 may not be able to stitch. A CT2 in surgery on their last day before ST3 might be able to perform a laparoscopic appendicectomy independently. Nonetheless, that guarantee of a minimal competence means that SHO will persist for some time.
Who dares wins?
Of course, what if you don’t enter a formal training programme? If you can’t get an ST3 job, are you destined to leave medicine? Firstly, you can locum but not everybody does this
The SAS grade (Staff grade and Associate Specialist) are folks who have done some specialist training but for whatever reason left the programme. They then work at about the level of an SpR but will not be offered formalised career progression.
Historically, staff grades would need sign-off from a specific number of consultants to progress to Associate Specialist. This meant a level of responsibility somewhere between consultant and SpR. Staff grades were often looked down upon as those not good enough to make it in training.
That perception was probably never accurate and is certainly well wide of the mark now. The two grades have been combined into “Specialty Doctor“, occasionally SD in the notes. In some trusts, Associate Specialists have kept their titles. In others, they have become Specialty Doctors but retain their pay from being Associate Specialists.
Other grades include:
Clinical Fellow: usually operating at junior but mostly middle grade level either with other responsibilities or are pursuing educational or academic goals whilst keeping a hand in clinical work.
Trust grade/trust doctor: usually doctors with temporary contracts working for a specific trust and not in training.
Post-CCT Fellow: doctors who have completed sufficient training to be consultants within their fields but wish to subspecialise. Normally on the middle grade rota, they will almost exclusively work in their specific field e.g. cardiac anaesthesia or children’s anaesthesia.
Age is just a number
Surely, the age of your doctor will give away how experienced they are? Oh, ye of little faith. A colleague of mine entered medicine at the age of 35. She was 17 years my senior. She would have been an F1 age 40. If I had taken no time out (and not failed a year of medical school), in a relatively long training programme, I’d be an anaesthetic consultant next year, age 33.
We already have an issue where women doctors are constantly referred to as nurses. Women more commonly than men seem to be told that they are “too young” to be a consultant despite all the requisite training. Perhaps it’s the facial hair but in 9 years as a doctor I have never, ever been told I looked too young or that I was nurse.
Also, the numbers in your grade are only years of training in that specialty. If, like many of my anaesthetic colleagues, you did two years of emergency medicine prior to anaesthetics, you’ve done two years of relevant training which your grade doesn’t reflect. Equally true if, like me, you did 18 months of part-time locums in amongst your training, this is not included. Nor is research (well, it might be) or education (actually that might be too).
Add in so-called less-than-full-time (LTFT) trainees, who might do 50-80% of the hours, it might take 12 months to do 6 months equivalent of training. Again, age will tell you little about how well trained your doctor is.
Conclusion
The difficulty is, the more flexible your grading system, the more accurate the descriptions to fellow medics but the less accurate it is to both fellow healthcare professionals and patients. The less flexible it is, the easier it is to understand to non-medics (and even some medics) but the less obvious it is what level of training somebody has.
(And to answer the question, “ACCS CT2 (AIM)” means “Acute Care Common Stem Core Trainee year 2 – (Acute Internal Medicine)” i.e. in their second year of the Acute Care Common Stem with a view to specialising in Acute Internal Medicine.)
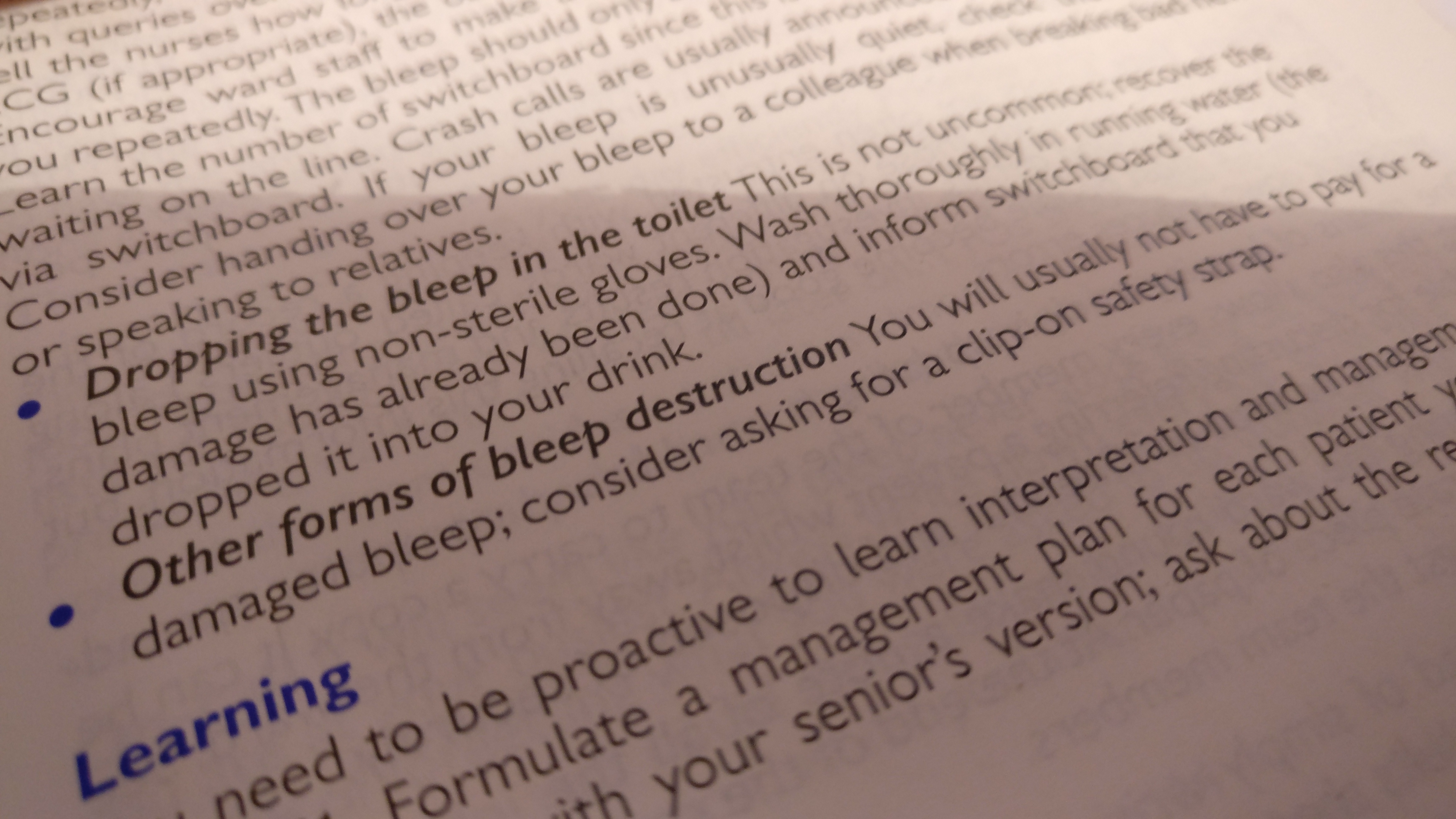
From the Oxford Handbook for the Foundation Programme (2nd edition) by Hurley, Dawson, Saunders & Eccles
In some sort of weirdly morbid onomatopoeia, the pagers which junior doctors carried all across the country are called “bleeps”. My Dad did his first house job in the UK in 1968 and they were introduced shortly afterwards. Up until that point, they had some weird light system which given my Dad has been telling the same 5 stories for about 50 years, you’d think I’d remember how it worked..
My bleep number as an F1 (Foundation Year 1 – first-year doctor) was 7144. If a nurse wanted to get in contact with me, they had to dial a prefix (let’s say 77), then the bleep number (7144), then the extension they were phoning from (let’s say 26723). So they’d dial 77 7144 26723. My bleep would bleep and the number “26723” would appear on my bleep. I would then find a phone, ring 26723 and they’d answer the phone.
There are significant advantages to this system. In the ten (I think) hospitals I’ve worked at over 9 years in the NHS, the system was roughly the same in each hospital. It worked throughout the hospital grounds (with one key exception). It’s been around so long, even the oldest, most technophobic staff understood how it work.
The actual bleeps themselves were fairly bulletproof. Whilst perhaps not as robust as the Nokia 3210 (it’s pronounced “thirty-two, ten” for you youngsters), you could certainly drop it without worry it was going to break. They rarely need batteries changing and the AA batteries they run off were readily available from switchboard.
It ain’t broke so, why fix it?
There are a whole bunch of issues with a bleep. By way of example:
You bleep somebody and they don’t bleep back – how long do you wait?
You get a bleep and phone back but get an engaged tone. Do you wait for the person to bleep you again or do you wait and then phone back on the same number?
You answer a bleep but nobody is picking up. How long do you wait before hanging up?
You bleep somebody but then the person that rings back isn’t the person you bleeped. You then have to go and find the person they’re ringing to speak to. Do you wait until that conversation is over or do you go and bleep from another phone? How long does the conversation have to go on for before you bleep from another phone?
You get two bleeps in a row. The second bleep wipes the number of the first bleep. You don’t know how to bring the first number back because there are three buttons on the bleep with icons you don’t understand.
You are seeing to a sick patient and get a bleep. There is nobody nearby. Do you leave the sick patient to answer, go and find somebody else to answer, or ignore it and hope they’ll bleep back.
Taking 30 minutes, sat in front of a phone, trying to contact somebody is a waste of everybody’s time. It has happened so many times in every doctor’s career.
Everybody’s got mobiles now, don’t they?
I spend a lot of time in theatres. Theatres are often in the basement of a hospital. As such, reception can often be very poor. Historically, hospitals restricted access to Wi-Fi (though this is largely changing); thus even Wi-Fi calling couldn’t get you through to people. Where Wi-Fi is available, this is useful for calling people but you can’t send anonymous patient data via messages.
Out-of-hours (OOH), it’s patently not feasible to have every doctor on internal medicine give their mobile phone out to every medical ward, especially if you’re covering multiple wards where you don’t normally work. And I wouldn’t be comfortable with my mobile being accessible to that many folks anyway.
What are the alternatives?
In terms of inter-doctor communication whilst on-call, now I’m on anaesthetics or ICU, I work in relatively small teams of doctors. For instance, when I worked at a tertiary children’s centre, there was me on-site and a consultant anaesthetist at home. Us having each other’s phone numbers worked well and we could actually text each other patient data as long as it didn’t use any specifics.
Hospital-at-night (now more accurately hospital-out-of-hours (OOH)) coordinators are wonderful things for bigger teams, particularly for the more junior junior doctors. They are nurse practitioners who triage OOH calls into job lists for doctors on-call.
Instead of an on-call junior having to stop to answer their bleep every time anybody needs them for something regardless of how urgent, they can work through their list overnight. It also means that sicker patients get triaged to more senior doctors by the nurses. Even in a world with mobiles which nurses could ring, it would clearly be frustrating if you got phoned every time you were needed.
Whilst I was an F1 in 2010-11, the hospital piloted Blackberries with an app which sent you your list of jobs. You ticked them off as you went along on the app and this let the OOH coordinator how busy you were. I assume it was more efficient; it was certainly less stressful.
Glorious! Let’s just switch it all online!
Woah, there. I’ve worked in hospitals where bleeping is online, ones where the nursing observations are online, ones with prescribing online, ones with notes online and currently work on an ICU where everything (with some minor if important exceptions) is computerised. Blood results and investigations are the only things which have been online in every hospital I’ve worked at.
A new system always come with problems. At one of the hospitals I worked at, the problem was there was a dead zone for bleeps. Unfortunately, it was on ICU where I, as the 2nd on-call for anaesthetics and ICU, covered crash Caesarean sections and paediatric arrests. If either went out, switchboard would have to ring ICU to ensure I wasn’t there.
They introduced a slightly bizarre system where the crash team carried mobile phones which said “cardiac arrest” when there was an arrest call (I think they’d set it as the ringtone). Being modern-ish mobile phones, the batteries didn’t last very long and even though there were (eventually) chargers and battery replacements, if you were busy and forgot your phone only had 30% charge, when you later went to put your head down for an hour, you might not realise it had run out before you woke up.
(They also introduced a replacement to the bleep system which relied on Google Hangouts. Unfortunately, Hangouts is due to be retired at the end of the year so, that’ll be fun for them. I thankfully don’t work there any more.)
All the systems I mention have had teething problems. The biggest issue is not user-friendliness (though that can be an issue, particularly for short-term or supply posts). It’s generally that the NHS usually has rubbish hardware. So even if you introduce your fancy new app, it doesn’t work.
So is Matt Hancock right?
To be honest, probably.
Whilst not an early adopter, I am quite happy trying new technology. The ICU system I mentioned earlier is the best NHS computer system I’ve used; indeed I and most of my colleagues agree that it is very likely to have saved lives. When I have to go back to ICUs that use paper, I just find the whole thing incredibly frustrating.
Computer systems are like any other system. There is an inevitable period of change. They need to be slowly but surely improved and updated. It will, frankly, probably be crap for at least the first 12 months.
But my question to folks who want to keep the bleep is this: would you be happy to return to paper blood results and films for X-rays? And if you’re not somebody who has to regularly bleep people, this probably isn’t the debate for you.
Like any government initiative, I await it with large and healthy doses of cynicism but this is a much more sensible challenge that Jeremy Hunt and Andrew Lansley who respectively took on junior doctors’ pay and the entire structure of the NHS.
Trying to get rid of bleeps seems a much more feasible and achievable goal, if for no other reason than a lot of trusts have made waves to do it. It just needs to be done right; that’s where I remain cynical of any government initiative.